What is a Labral Tear?
The labrum is a ring of strong cartilage that lines the rim of the shoulder socket (glenoid).
Its function is to deepen the socket and provide stability — much like a cushion that holds the ball of the humerus firmly in place.
When this cartilage ring is torn, it is called a labral tear.
Depending on the site of tear, it can cause pain, clicking, catching, locking, or instability of the shoulder joint.
Labral tears are often associated with athletes, especially those involved in throwing, overhead, or contact sports — but can also occur from falls, accidents, or even chronic overuse.
⚙️ How Does it Develop?
The labrum can tear either due to a sudden traumatic injury or gradual repetitive stress on the shoulder.
- In younger patients or athletes, it’s commonly from repetitive overhead activity (like throwing, swimming, or weightlifting).
- In older adults, it can result from degeneration or wear and tear of the shoulder joint.
A labral tear often coexists with other injuries such as rotator cuff tears or shoulder instability.
🧩 Types of Labral Tears
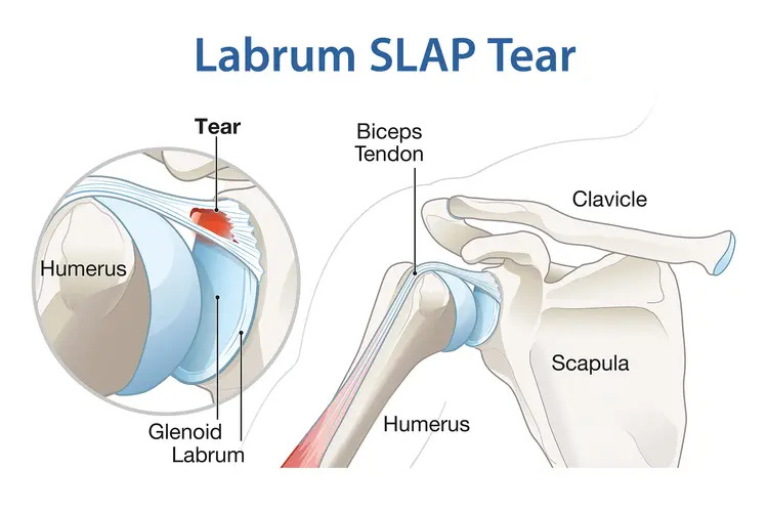
1. SLAP Tear (Superior Labrum Anterior to Posterior)
- The tear occurs at the top (superior) part of the labrum — where the biceps tendon attaches.
- It extends from the front (anterior) to the back (posterior) of the superior labrum.
- Commonly seen in throwing athletes, gym enthusiasts, and those with repetitive overhead motion.
- Symptoms: Clicking, pain with overhead activities, weakness, and decreased throwing velocity.
2. Bankart Lesion
- Involves detachment of the anteroinferior (front-bottom) labrum — usually after a traumatic shoulder dislocation.
- Causes recurrent instability or the sensation that the shoulder may “pop out.”
3. Posterior Labral Tear
- Less common; occurs after posterior shoulder dislocation or repetitive stress in contact athletes (wrestlers, weightlifters).
⚠️ Risk Factors
- Repetitive overhead or throwing sports (cricket, baseball, volleyball)
- Traumatic shoulder dislocation
- Sudden heavy lifting or jerky pulling movement
- Poor shoulder mechanics or instability
- Age-related degeneration
- Inadequate rehabilitation after prior shoulder injury
🔬 Etiology & Pathophysiology
The labrum can be injured through traction (pulling of the biceps tendon), compression (falling on an outstretched arm), or shear stress (repetitive overhead movements).
In SLAP lesions, repetitive torsional stress on the long head of biceps tendon detaches the labrum from the glenoid rim.
In Bankart lesions, the labrum and capsule tear off after anterior dislocation, compromising joint stability.
Both types result in a loss of the “suction cup effect” of the shoulder — leading to instability and pain.
🧪 Investigations
- Clinical Examination:
- O’Brien’s test, Crank test, and Biceps Load test may reproduce symptoms.
- Apprehension and Relocation tests help identify associated instability.
- Imaging:
- X-ray: Usually normal but rules out fractures or calcifications.
- MRI / MR Arthrogram:
- Gold standard for visualizing labral tears and biceps anchor detachment.
- MR arthrogram increases accuracy by highlighting small tears with contrast.
💊 Management
🩹 Non-Surgical (For Minor / Degenerative Tears)
- Rest, activity modification, and physiotherapy focusing on scapular and rotator cuff strengthening.
- Anti-inflammatory medications for pain relief.
- Ultrasound-guided injections (PRP or corticosteroid) may help in inflammation control.
- Regular follow-up to assess stability and functional recovery.
🩺 Surgical (For Symptomatic or Instability-Associated Tears)
- Arthroscopic Labral Repair:
- Minimally invasive keyhole surgery to reattach the torn labrum using bio-anchors.
- SLAP Repair:
- Anchors re-fix the superior labrum and stabilize the biceps tendon attachment.
- Biceps Tenodesis (in select cases):
- The biceps tendon is reattached outside the joint to relieve tension on the labrum — especially effective in older patients or revision cases.
- Rehabilitation Protocol:
- Sling immobilization for 3–4 weeks.
- Gradual range-of-motion exercises, followed by strength and sports-specific training.
⏳ Sequelae if Left Untreated
- Persistent pain and mechanical clicking
- Progression to recurrent shoulder instability
- Secondary rotator cuff or biceps tendon injury
- Labral degeneration leading to early arthritis
- Decreased athletic performance and reduced throwing power
🌟 Prognosis
With precise arthroscopic repair and guided physiotherapy, most patients regain full function and return to sports within 4–6 months.
Success rates exceed 90%, with excellent pain relief and restoration of shoulder stability.
💬 Key Takeaway
“A labral tear may be invisible on X-rays, but not on your performance — early diagnosis and keyhole repair restore your shoulder’s natural stability and power.”