What is Shoulder Dislocation & Instability?
The shoulder joint is the most mobile joint in the human body — and also the most prone to dislocation.
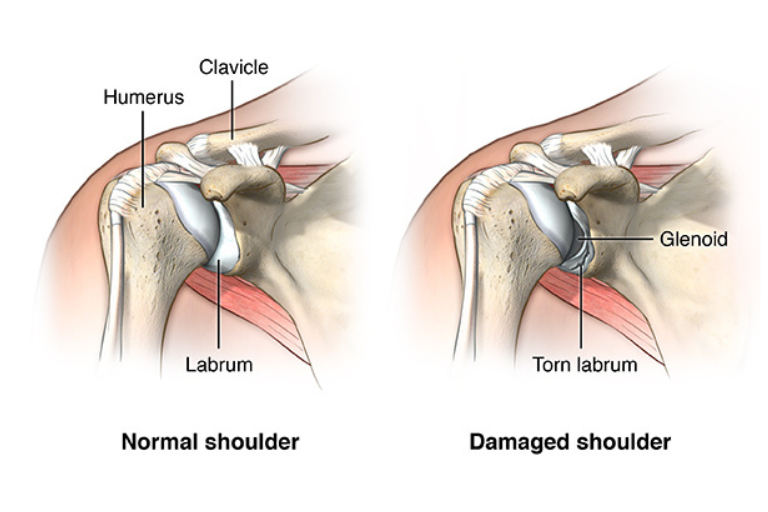
A shoulder dislocation occurs when the head of the humerus (arm bone) slips out of its socket (glenoid).
When this happens repeatedly, or the shoulder constantly feels like it’s “slipping out” during daily activities or sports, it is termed shoulder instability.
Patients typically describe a feeling of insecurity or “giving way” of the shoulder while throwing, lifting, or even sleeping on that side.
⚙️ How Does it Develop?
Shoulder instability develops either after a single major traumatic event or due to gradual stretching and weakness of stabilizing structures over time.
- Traumatic Instability:
Often follows a single, forceful injury — such as a fall or tackle — causing tearing of stabilizing tissues (e.g., labrum or ligaments). - Atraumatic Instability:
Caused by repetitive microtrauma in athletes (like swimmers, gymnasts, and throwers) or in people with naturally loose ligaments (hypermobility).
The joint loses its balance between mobility and stability — making it prone to further dislocations, sometimes with even minor movements.
⚡ Types of Shoulder Instability
- Anterior Instability (most common)
- The humeral head moves forward out of the socket.
- Usually occurs with the arm in an abducted and externally rotated position (e.g., while throwing).
- Posterior Instability
- The humeral head moves backward, commonly seen after seizures or electric shock injuries.
- Multidirectional Instability (MDI)
- Shoulder becomes loose in more than one direction due to generalized ligament laxity.
- Common in young females and athletes with hypermobile joints.
⚠️ Risk Factors
- History of previous dislocation
- Contact or overhead sports (cricket, volleyball, basketball, swimming)
- Generalized ligament laxity or hypermobility
- Poor rehabilitation post initial dislocation
- Genetic connective tissue disorders
- Repeated microtrauma in overhead athletes
🔬 Etiology & Pathophysiology
When the shoulder dislocates, several structures may get injured:
- Labral Tear (Bankart Lesion): The fibrocartilage rim (labrum) that deepens the socket tears away.
- Capsular Stretching: The ligaments and capsule become loose, reducing joint stability.
- Hill-Sachs Lesion: Impression fracture on the humeral head caused by impact against the glenoid rim during dislocation.
- Bony Bankart: A fragment of the glenoid bone breaks off along with the labrum.
Each subsequent dislocation worsens these lesions, further destabilizing the joint — a vicious cycle if not corrected.
🧪 Investigations
- Clinical Examination:
- Apprehension and Relocation Tests for anterior instability.
- Load & Shift Test, Sulcus Sign for multidirectional instability.
- Imaging:
- X-ray: To confirm direction of dislocation and rule out fractures.
- MRI / MR-Arthrogram: To visualize labral, capsular, and bony lesions.
- CT Scan (3D): For pre-operative assessment of bone loss on humeral head or glenoid.
💊 Management
🩹 Non-Surgical
- First-time dislocation (without fracture):
- Immediate reduction, short immobilization, followed by guided physiotherapy.
- Focus on strengthening rotator cuff and scapular stabilizers.
- Atraumatic / Multidirectional Instability:
- Structured physiotherapy emphasizing proprioception, posture correction, and muscle balance.
🩺 Surgical
If instability recurs or significant labral/bony damage is present:
- Arthroscopic Bankart Repair:
- The torn labrum and capsule are reattached to the glenoid using anchors.
- Restores the natural “bumper effect” of the shoulder socket.
- Remplissage / Capsular Shift:
- Address associated Hill-Sachs lesions and tighten stretched capsule.
- Latarjet Procedure:
- For cases with significant bone loss — transfers a piece of coracoid bone to reinforce the socket and prevent re-dislocation.
- Rehabilitation Protocol:
- Arm sling for 3–4 weeks post-surgery.
- Gradual physiotherapy to restore motion and strength.
- Return to sports typically by 4–6 months.
⏳ Sequelae if Left Untreated
Neglected or recurrent shoulder instability can lead to:
- Repeated dislocations with minor movements
- Progressive bone loss on glenoid or humeral head
- Chronic pain and weakness
- Loss of athletic performance
- Post-instability arthritis (glenohumeral arthropathy) over time
- Irreversible damage requiring complex reconstruction or shoulder replacement
🌟 Prognosis
With proper diagnosis, advanced arthroscopic repair, and structured rehabilitation, recurrence rates drop below 5–10%, and most patients resume full activity without fear of dislocation.
💬 Key Takeaway
“Once a shoulder dislocates, it becomes easier for it to slip out again — but modern arthroscopic techniques can restore stability, confidence, and performance.”