What is Shoulder Impingement Syndrome?
Shoulder Impingement Syndrome is one of the most frequent causes of shoulder pain, particularly in individuals who perform repetitive overhead movements — athletes, gym-goers, painters, and desk workers alike.
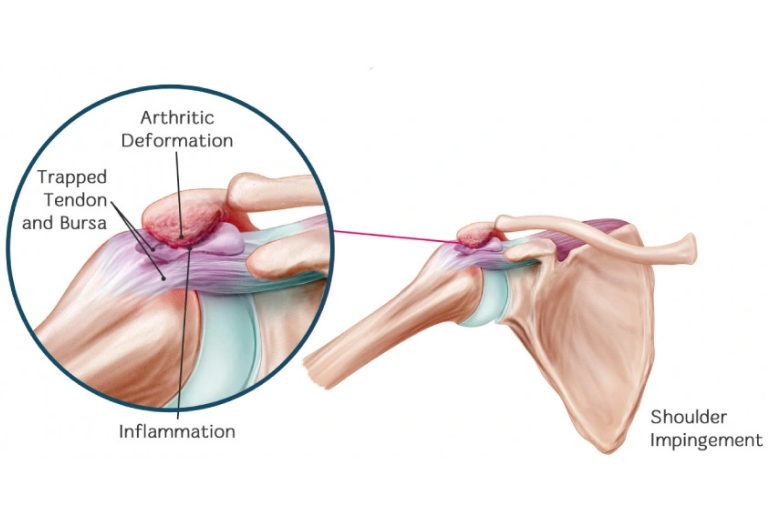
It occurs when the rotator cuff tendons or bursa get repeatedly “pinched” between the upper arm bone (humerus) and the outer edge of the shoulder blade (acromion).
This repeated friction leads to inflammation, pain, and eventually weakness of the shoulder.
Patients typically complain of pain while lifting the arm overhead, difficulty wearing clothes, or discomfort during night sleep on the affected side.
⚙️ How Does it Develop?
The shoulder joint is designed for maximum mobility, but this comes at the cost of stability.
When the shoulder mechanics are altered — due to poor posture, muscle imbalance, or repetitive strain — the rotator cuff tendons get compressed during motion.
Over time, this repeated pinching leads to inflammation of the bursa (bursitis) and tendons (tendinitis), causing pain and restricted movement.
🧩 Types of Shoulder Impingement
1. External (Subacromial) Impingement
- The most common type.
- Occurs outside the joint, where the rotator cuff tendons and subacromial bursa are trapped between the humeral head and the acromion.
- Common causes: bone spurs, acromial shape (hooked acromion), or thickened bursa.
- Seen in middle-aged individuals and overhead athletes.
2. Internal (Posterosuperior) Impingement
- Occurs inside the joint, where the undersurface of the rotator cuff rubs against the glenoid rim or labrum during extreme external rotation and abduction.
- Typically seen in throwing athletes (cricketers, baseball players, swimmers).
- It is a subtle, high-demand injury linked with shoulder instability and labral pathology.
⚠️ Risk Factors
- Repetitive overhead activity (sports or occupation)
- Poor posture (forward head and rounded shoulders)
- Weak scapular stabilizers or core muscles
- Imbalance between rotator cuff and deltoid
- Bone spurs or acromial morphology (hooked acromion)
- Previous shoulder injury or instability
🔬 Etiology & Pathophysiology
External Impingement:
Due to narrowing of the subacromial space by bone spurs, bursal inflammation, or thickened rotator cuff tendons. The repeated contact leads to tendon wear and micro-tears, eventually progressing to partial or complete rotator cuff tears.
Internal Impingement:
Caused by repetitive overhead external rotation, especially in throwing athletes, where the humeral head translates posteriorly, leading to friction between the cuff’s undersurface and the posterosuperior glenoid rim. Chronic cases show partial articular-sided cuff tears and labral fraying.
🧪 Investigations
- Clinical Examination:
- Painful arc, Neer’s test, Hawkins–Kennedy test, and Jobe’s test.
- Imaging:
- X-ray: To detect bone spurs or acromial morphology.
- Ultrasound: Shows bursitis or tendon inflammation.
- MRI: Confirms impingement, tendon status, and associated labral or bursal pathology.
💊 Management
🩹 Non-Surgical Management
- Activity modification and posture correction
- Physiotherapy focused on scapular control, rotator cuff strengthening, and stretching of pectoral muscles
- Anti-inflammatory medication or ultrasound-guided corticosteroid/PRP injection for persistent bursitis
- Ergonomic and sports-specific retraining
🩺 Surgical Management
If conservative measures fail after 3–6 months:
- Arthroscopic Subacromial Decompression: Removal of inflamed bursa and bone spurs to enlarge the subacromial space.
- Addressing Associated Lesions:
- Repair of partial-thickness rotator cuff tears
- Treatment of labral or internal impingement lesions
- Early physiotherapy ensures full restoration of motion and strength.
⏳ Sequelae if Left Untreated
If not addressed early:
- External Impingement → progression to chronic bursitis, partial/full rotator cuff tear, and eventually cuff tear arthropathy.
- Internal Impingement → may lead to labral tears, posterior shoulder instability, and irreversible cuff degeneration.
Ultimately, shoulder function deteriorates, causing persistent pain, weakness, and difficulty with daily activities and sports.
🌟 Prognosis
With early diagnosis and targeted rehabilitation, most patients recover fully and return to sports or work without restrictions.
Advanced arthroscopic techniques ensure minimally invasive correction with faster recovery.
💬 Key Takeaway
“Pain in your shoulder during overhead activity isn’t just fatigue — it could be the first sign of impingement.
Early correction restores strength, mobility, and prevents long-term tendon damage.”